QUALITY OF LIFE ANALYZED IN
PATIENTS TREATED WITH TYSABRI
TYSABRI can produce clinically meaningful improvements in mental and social health1
MS PATHS (Multiple Sclerosis Partners Advancing Technology and Health Solutions) was an initiative conducted in 10 healthcare institutions in 3 countries, each contributing standardized patient data during routine office visits from a large real-world cohort of MS patients. This analysis investigated the experiences reported by patients after starting natalizumab (n=164) using Quality of Life in Neurological Disorders (Neuro-QoL) assessments of 12 domains related to physical, mental, and social health. In Neuro-QoL, standardized
T-scores for each domain are derived from patient responses on a 5-point scale related to their feelings or functioning in the prior 7 days.
- The change in Neuro-QoL T-scores for each domain was assessed with a multivariate-adjusted mixed effects regression model
- Clinically meaningful change for each domain was defined as a ≥5-point change (≥0.5 standard deviation [SD]) in T-score from baseline. The percentage of patients with clinically meaningful improvement or worsening in T-scores was calculated from the last available Neuro-QoL
- In addition to the overall population, analyses were also conducted in patients with impairment in Neuro-QoL domains at baseline, defined as a T-score of ≥55 for each of the negatively worded domains or ≤45 for each of the positively worded domains
Study limitations:
- This is a real-world study that lacks randomization, and the results thus may be impacted by unconsidered variables or incomplete adjustment
- The standard cutoff of 5 points or half of standard deviation was used to establish minimal clinically important difference. The cutoff was based on the estimated effect size from several studies that included a mixed population of patients with diverse chronic diseases as well as some patients with MS
CHANGES IN NEURO-QoL DOMAINS IN PATIENTS TREATED WITH TYSABRI1
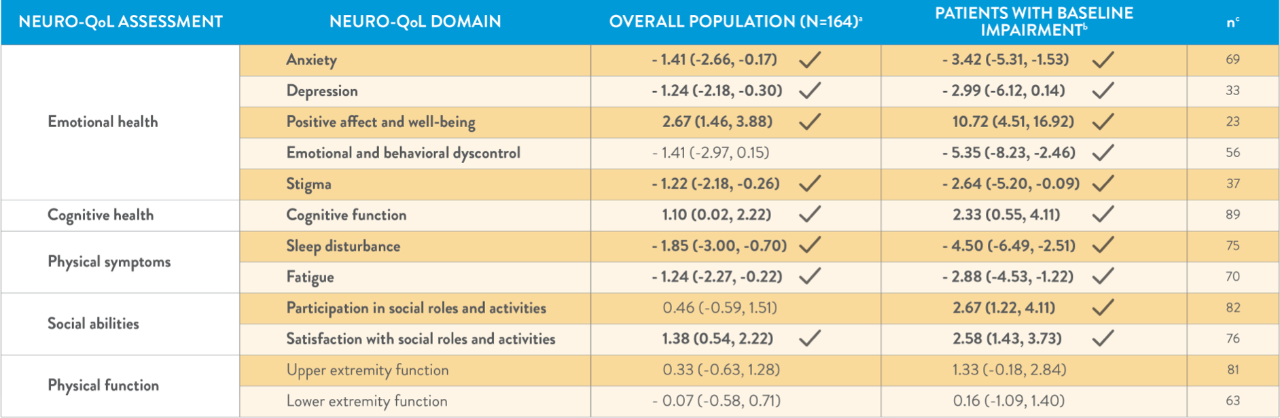
aDue to reconfiguration of the MSPT during the course of this study, 14 of the 164 patients did not provide responses to 2 of the Neuro-QoL domains—(1) positive affect and well-being and (2) emotional and behavioral dyscontrol—resulting in a total of 150 individual patient responses for these 2 domains.
bBaseline Neuro-QoL impairment was defined as a T-score ≥55 for negatively worded domains or T-score ≤45 for positively worded domains.
cNumber of patients with baseline impairment.
MSPT=Multiple Sclerosis Performance Test.
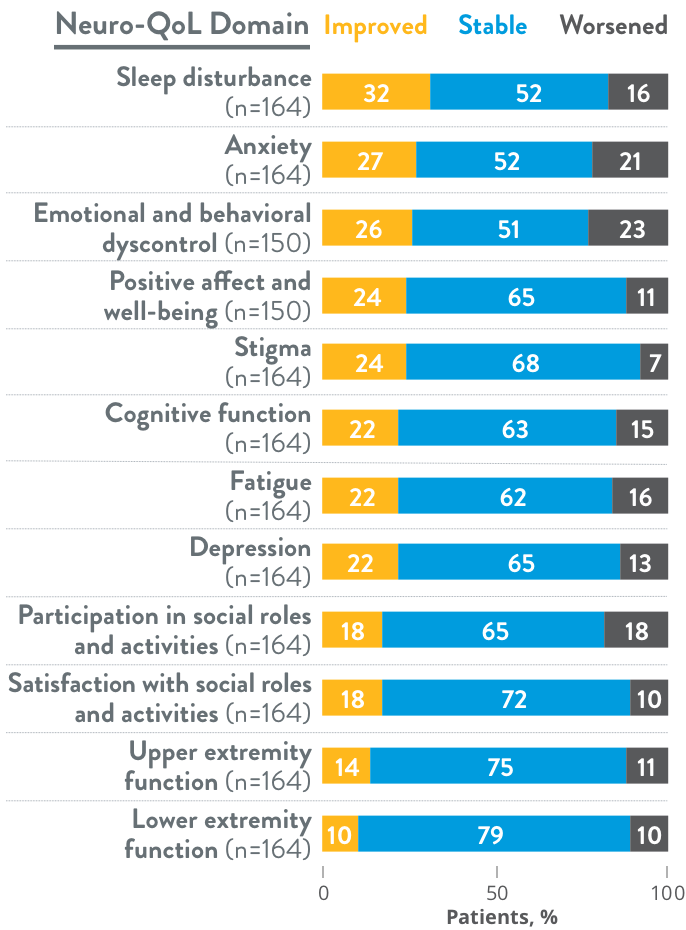
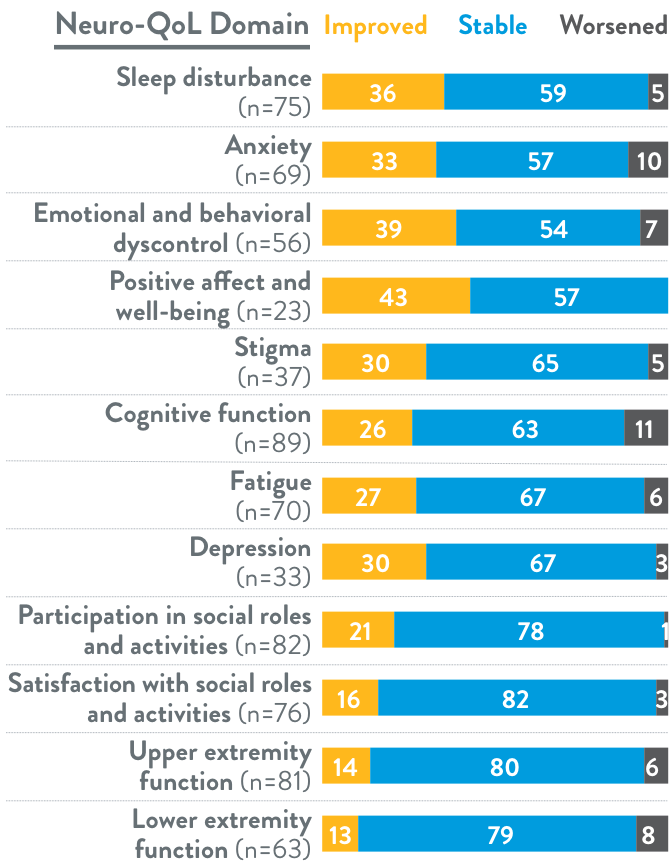
>75% of patients in the overall population improved or remained stable across each
of the assessed domains
CLINICALLY MEANINGFUL CHANGE IN NEURO-QoL T-SCORES
(OVERALL POPULATION)1
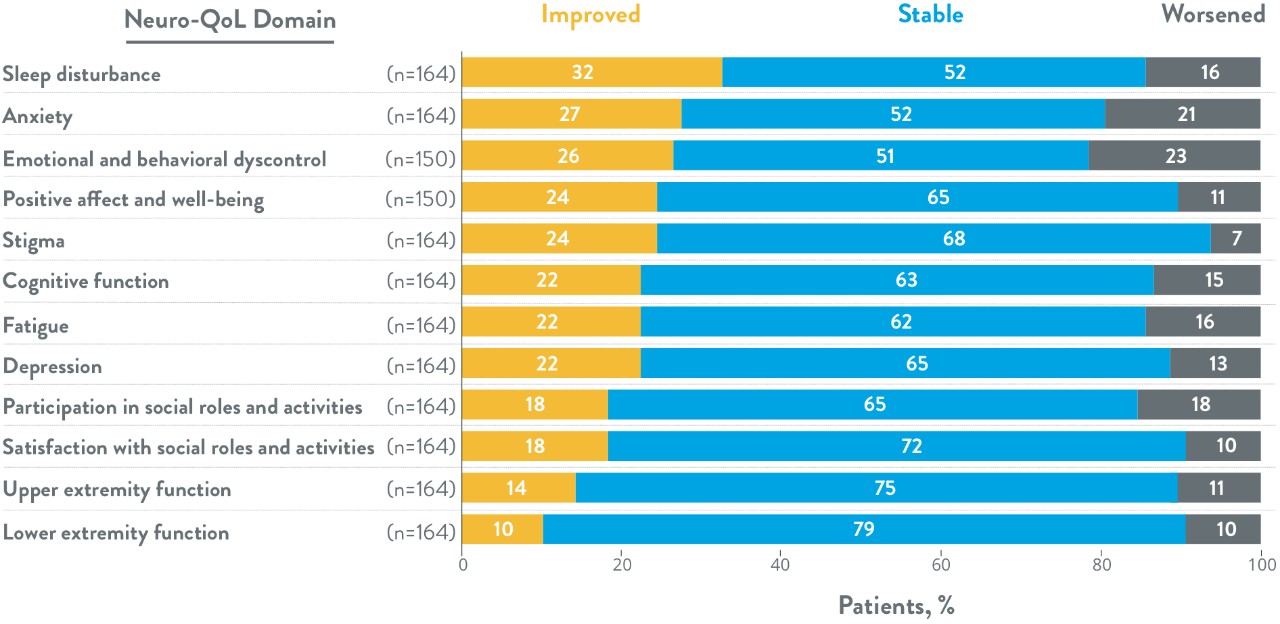
- 89% of patients improved or remained stable on the positive affect and well-being domain
- 85% of patients improved or remained stable on the cognitive function domain
- 84% of patients improved or remained stable on the fatigue domain
≥89% of patients with baseline impairment improved or remained stable across each
of the assessed domains
CLINICALLY MEANINGFUL CHANGE IN NEURO-QoL T-SCORES
(BASELINE IMPAIRMENT POPULATION)1
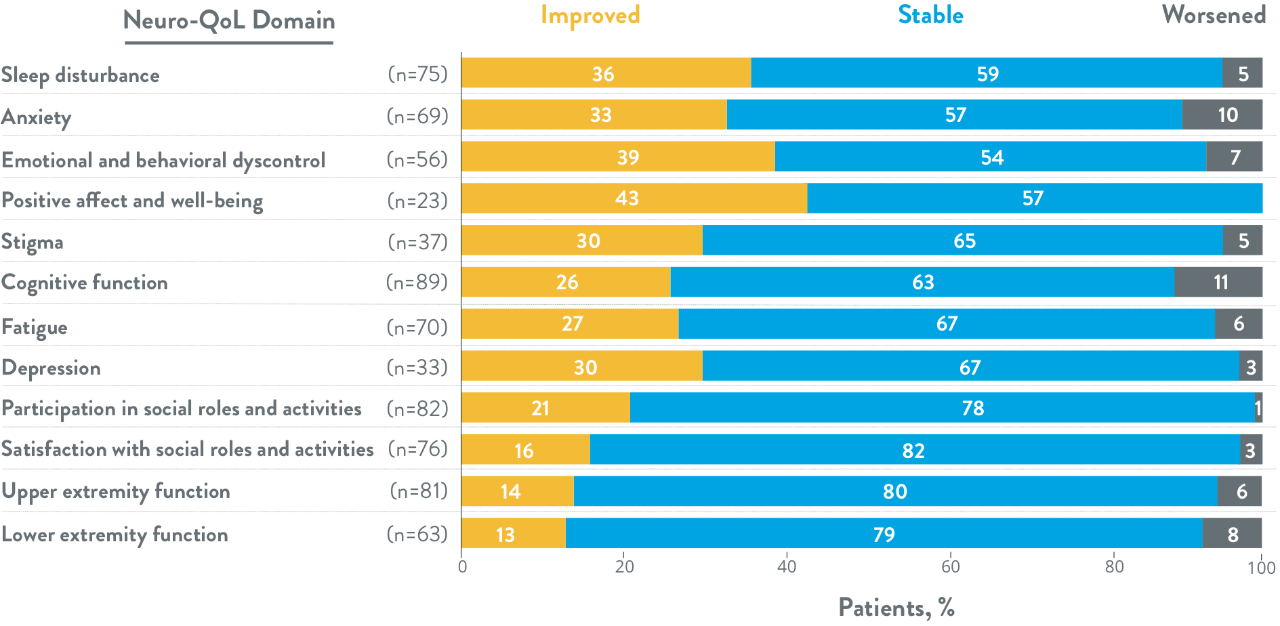
- 100% of patients improved or remained stable on the positive affect and well-being domain
- 89% of patients improved or remained stable on the cognitive function domain
- 94% of patients improved or remained stable on the fatigue domain
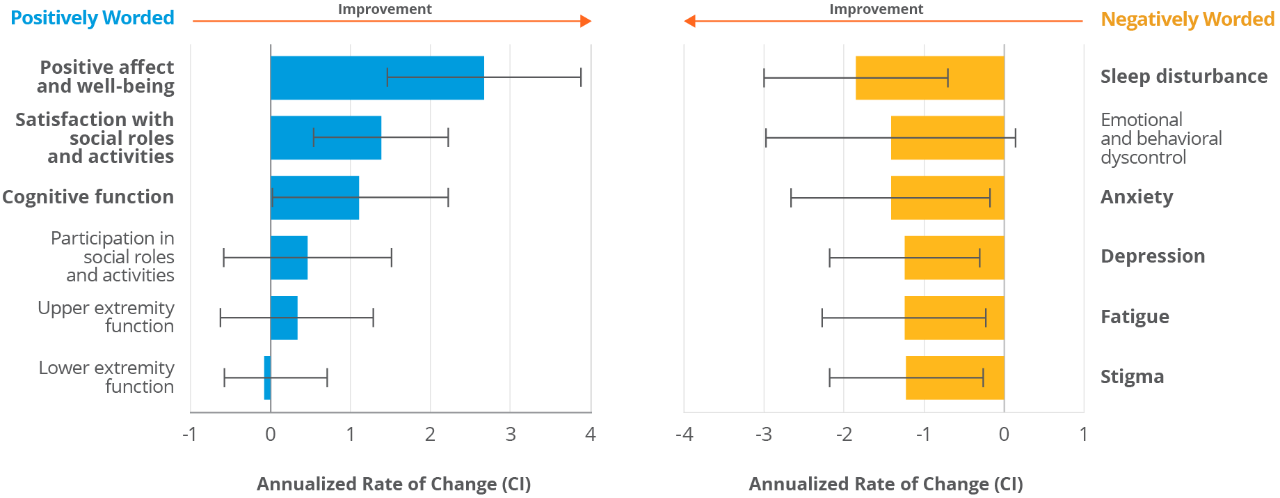
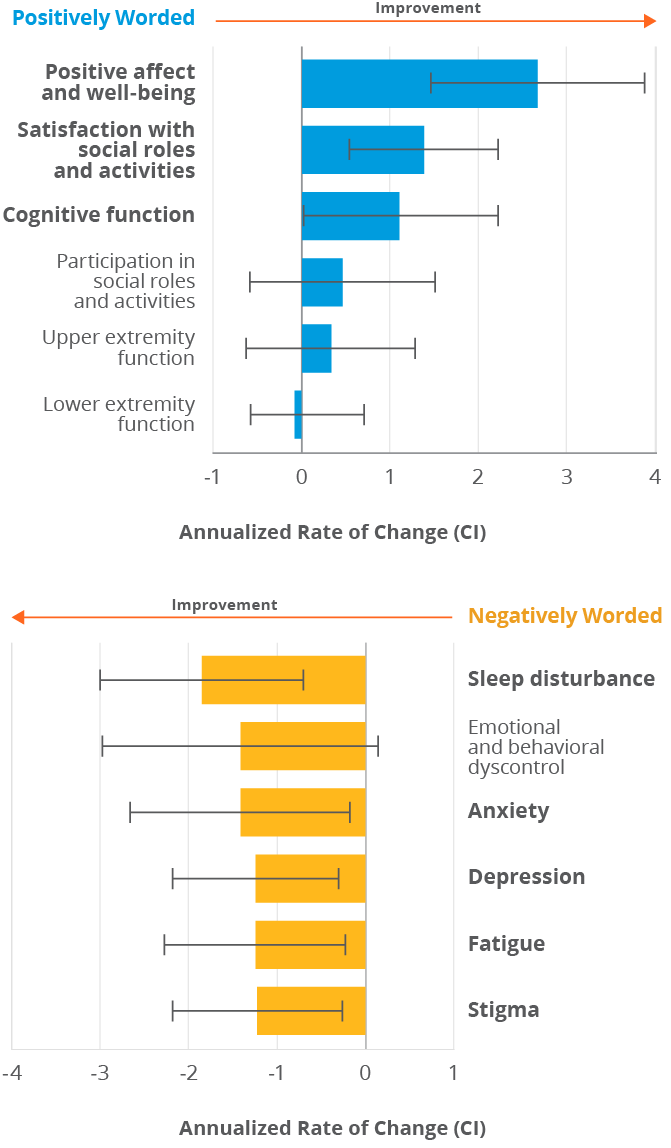
Patients treated with TYSABRI in the overall population improved in 8 of 12 Neuro-QoL domains vs baseline1
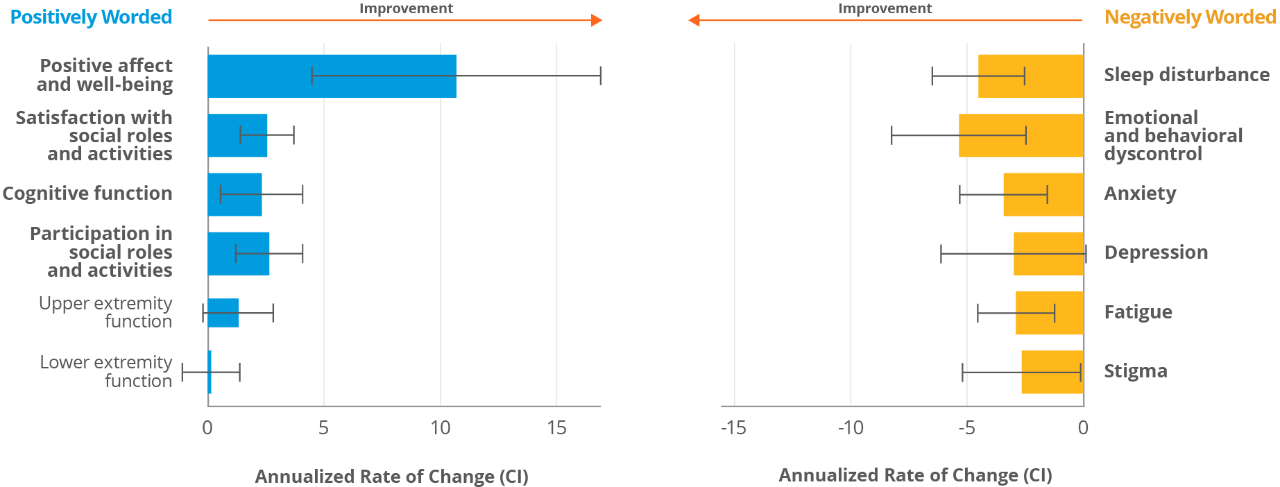
Patients treated with TYSABRI who had baseline Neuro-QoL impairment improved in 10 of 12 domains1
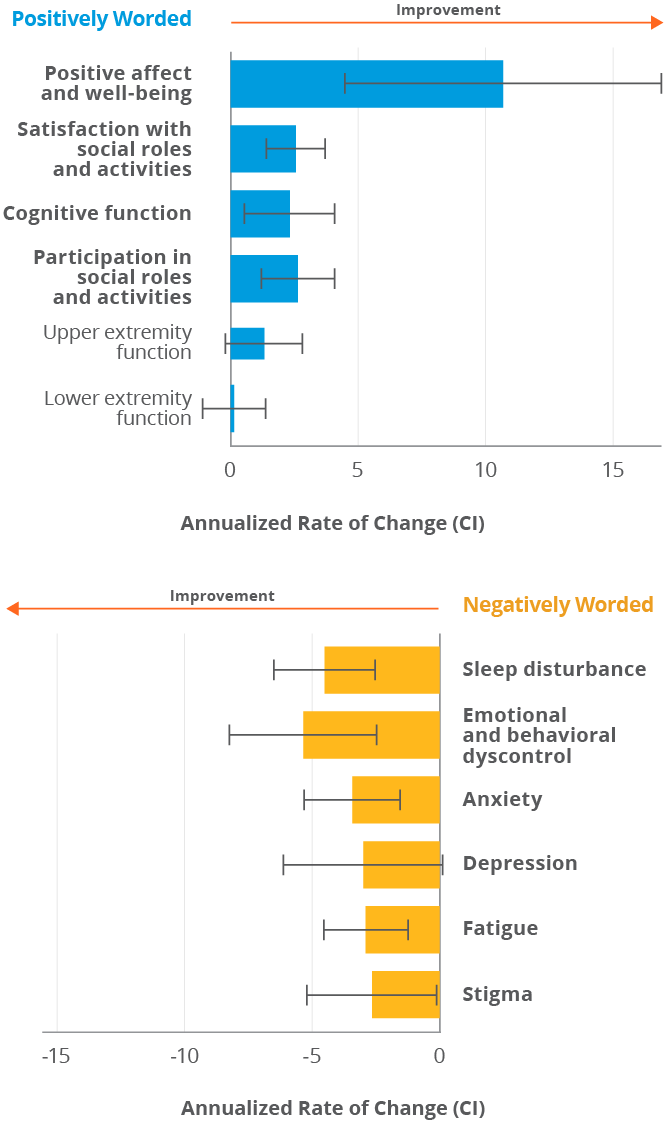
Bold rows indicate that more patients achieved clinically meaningful improvement than worsening.
- A greater proportion of patients treated with TYSABRI in the overall population reported clinically meaningful improvement than worsening for all domains except lower extremity function and participation in social roles and activities, for which an equal number of patients worsened and improved