LONG-TERM OBSERVATIONAL STUDY
OF OVER 6000 PATIENTS
REAFFIRMS
THE
TYSABRI SAFETY
PROFILE1
Study description: The TYSABRI Observational Program (TOP) was an open-label, multinational, multicenter, prospective study observing 6148 patients with RRMS outside of the US receiving 300 mg TYSABRI IV every 4 weeks for 15 years in real-world clinical practice settings. Of the 6148 patients enrolled, 3210 patients discontinued TYSABRI, and 2117 withdrew from TOP. Of the 3210 patients who discontinued TYSABRI treatment, 1093 remained in TOP. RRMS patients enrolled in TOP were required to be TYSABRI-naive or have received ≤3 doses of TYSABRI in their lifetime. This 10-year interim analysis includes data from study initiation (July 2007) through November 1, 2017.1,2






Study limitations1:
- The study is observational, without randomization or a placebo control group
- Attrition bias is inherent in long-term observational studies. Analysis of attrition bias is limited by the small number of patients in the <8-year treatment group, which decreased from 1056 at baseline to 389 at 8 years. The decrease occurred at various time points, resulting in varied treatment durations
- Results should be interpreted with caution, as treatment practices vary by country
The longest evaluation of real-world outcomes in patients treated with TYSABRI to date
- In 2007, Biogen initiated TOP, which assessed real-world safety and efficacy outcomes in patients treated with TYSABRI across the globe
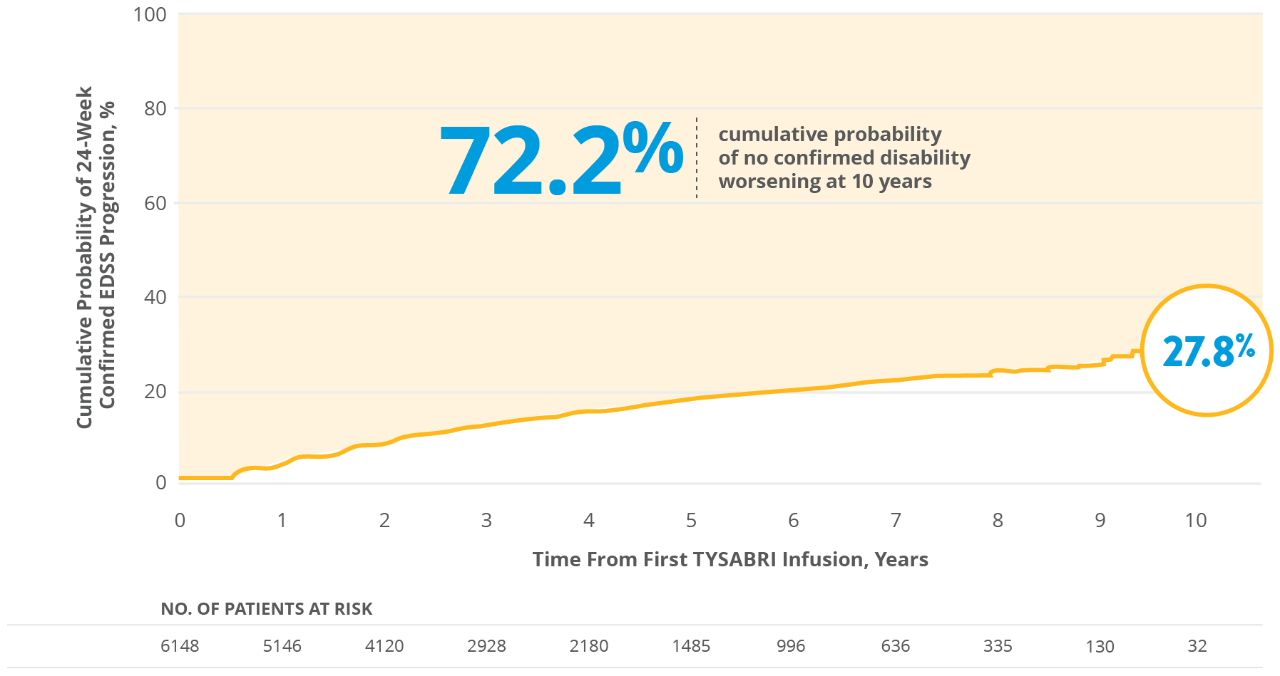
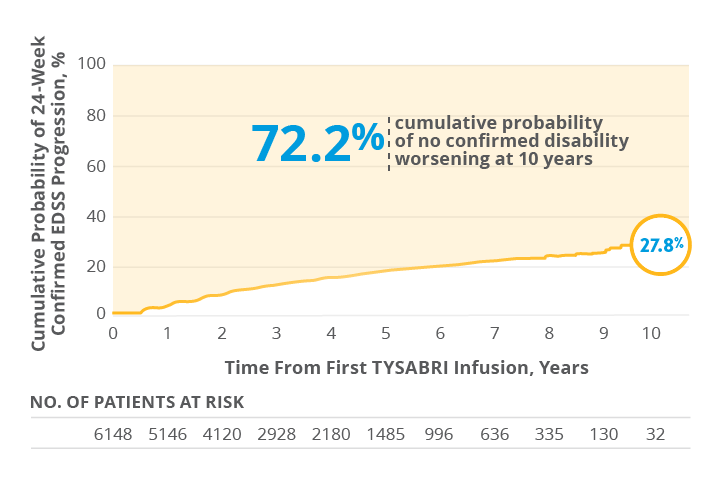
TYSABRI had a sustained impact on disability progression and ARR out to 10 years1,a
Copyright © 2020 Butzkueven H, et al; licensee BMJ is adapted under CC BY-NC.
aCumulative probability of confirmed disability worsening was defined as an increase of ≥1.5 from a baseline EDSS score of 0.0, ≥1.0 from a score of ≥1.0 to <6.0, or ≥0.5 from a score of ≥6.0, sustained for 24 weeks.1
Median EDSS scores were stable over 10 years
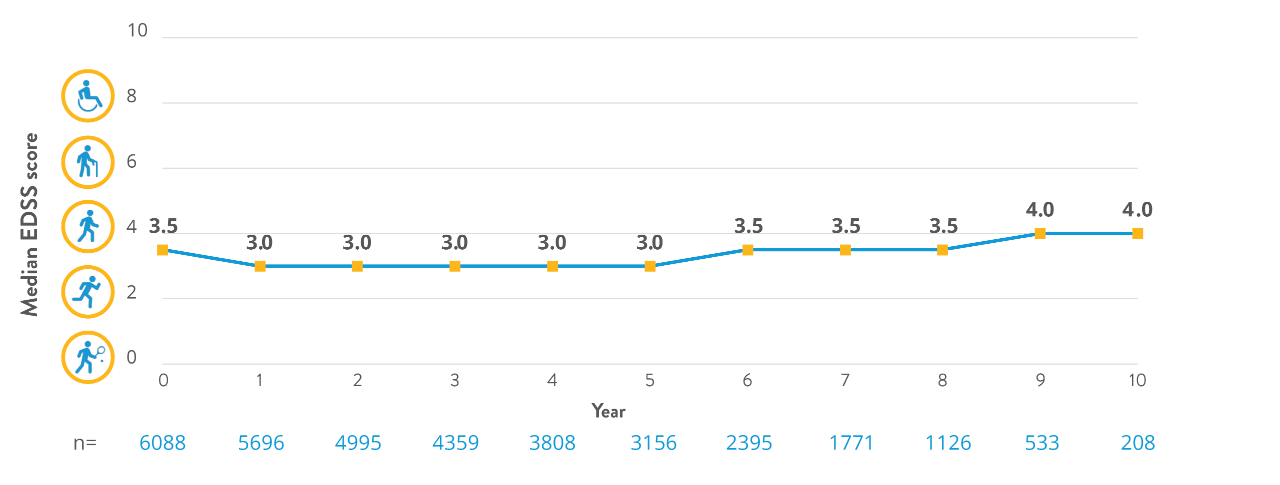
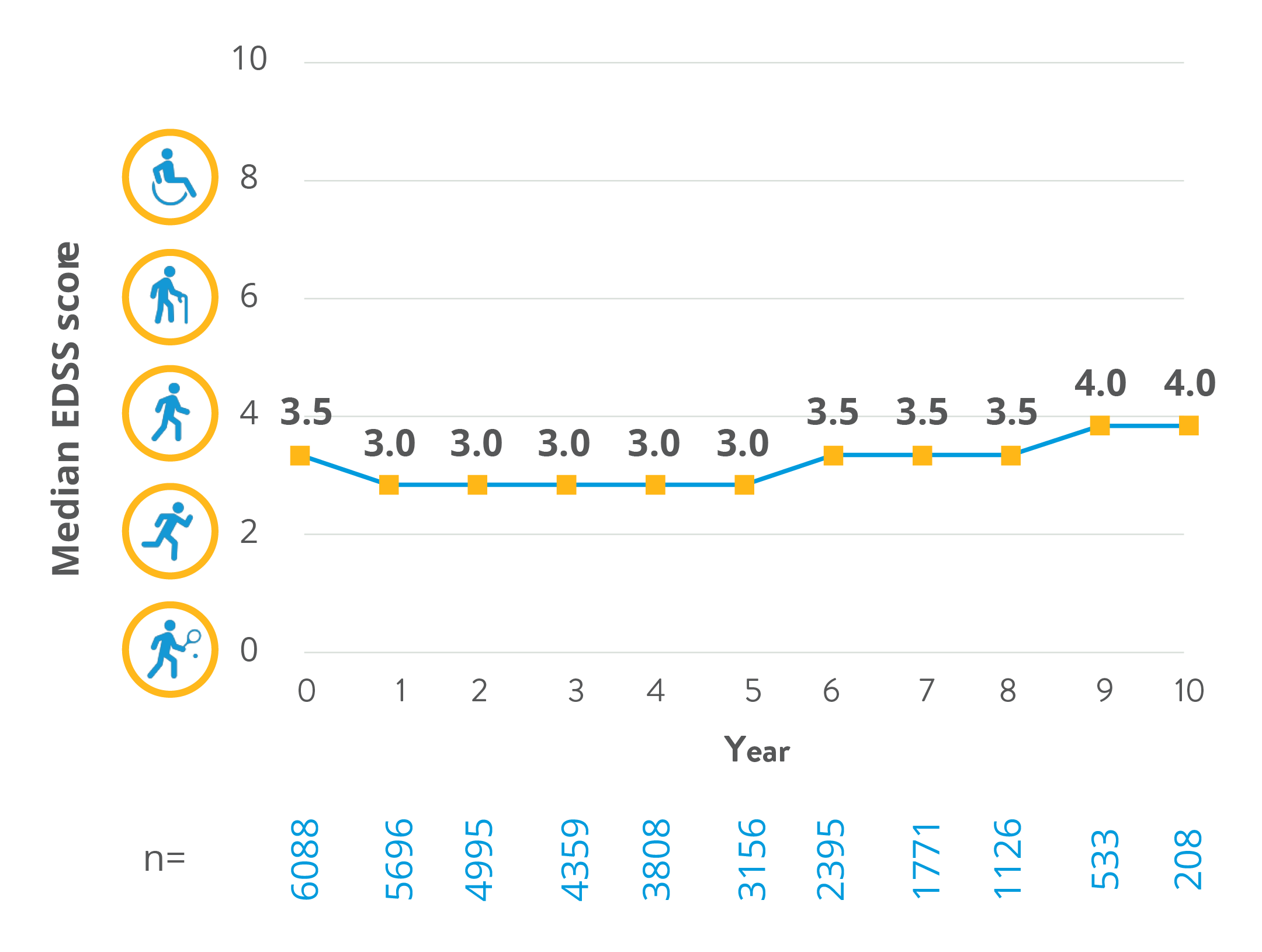
- At Year 10, very few patients were eligible to be counted due to disability progression measurements (which had to verify sustained progression 6 months after detecting progression), low initial enrollment, and treatment discontinuations
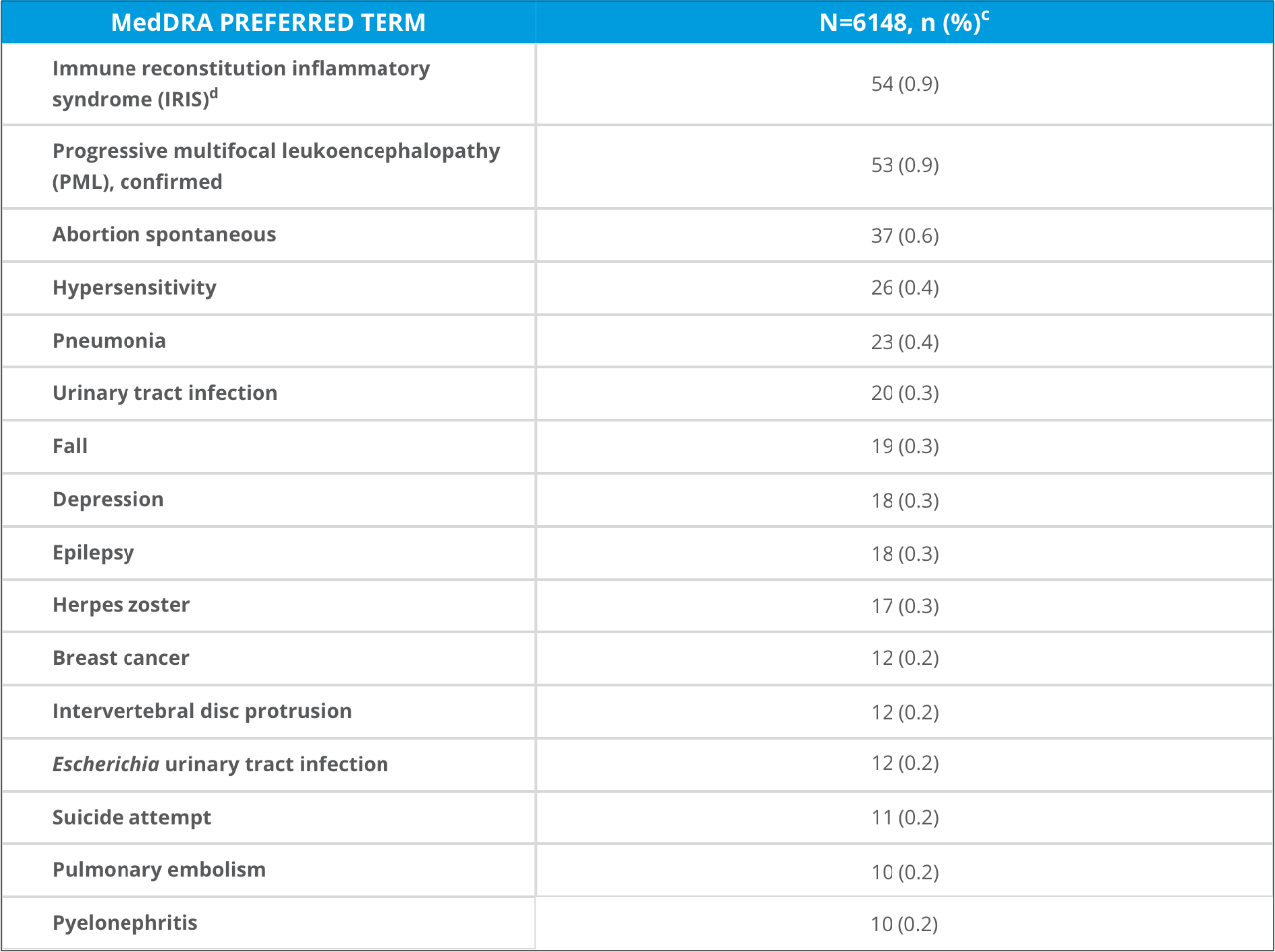
>85% of patients receiving TYSABRI experienced no SAEs in the 10-year TOP study1
INCIDENCE OF SELECT SAEs OCCURRING IN ≥10 PATIENTS IN TOP

Copyright © 2020 Butzkueven H, et al; licensee BMJ is adapted under CC BY-NC.
bEach patient was counted only once within each preferred term.1
cOne case of IRIS was not associated with PML.1
- SAEs related to hypersensitivity reactions (n=40, 0.7% of patients) included anaphylactic reaction (n=4), anaphylactoid reaction (n=3), anaphylactic shock (n=5), and hypersensitivity (n=28)
- 12 hepatic events (0.2% of patients) were reported during the study
- 30 deaths (0.5%) were reported during the study
- Physicians classified 8 deaths as treatment related, which included PML (n=4), IRIS (n=2, one of which was combined with MS relapse), metastatic breast cancer (n=1), and autonomic nervous system imbalance (n=1)
Incidence rates for opportunistic infections, malignancy, and PML were low (~1%)1
SERIOUS ADVERSE EVENTS OF INTEREST


Copyright © 2020 Butzkueven H, et al; licensee BMJ is adapted under CC BY-NC.
dBased on the time from the first dose of natalizumab until the last natalizumab dosing date + 6 months.1
eCalculated as (1000 × number of patients with an event) / (total patient-years of follow-up).1
fExact CIs are calculated based on the Poisson distribution.1
- Results are in line with the current understanding of the risk factors for PML
- Prior immunosuppressant use was reported by 26.4% of patients with PML
- 97.2% of PML cases (35 out of 36) with reported anti-JCV antibody serostatus 6 months prior to PML development were confirmed positive
- JCV antibody status was not tested at enrollment in 1809 out of 6148 patients (29.4%) and was missing from 7 patients who were tested at enrollment (0.1%)
- 67.9% of PML cases (36 out of 53) occurred in patients receiving TYSABRI for >3 years
- Overall, there were 66 patients with 39 types of malignancies
- Incidence of breast cancer was 0.3% (19 of 6148 patients), or 86.7 per 100,000 patient-years taking TYSABRI (95% CI: 52.2-135.4 per 100,000 patient-years)
The TOP Study was funded by Biogen.